Page created 6.i.19 from material on old psyctc.org site first mounted 5.viii.96.
Contents
Background and introduction
This is a one page, 22 item questionnaire which I designed in the light of a literature review resulting in a paper done in the days before “systematic reviews” :
Lacey & Evans (1986) The Impulsivist: a multi-impulsive personality disorder British Journal of Addiction 81:641-649.
https://doi.org/10.1111/j.1360-0443.1986.tb00382.x.
It was also influenced by some work reported in:
Evans & Lacey (1992) Multiple self-damaging behaviour among alcoholic women. A prevalence study. British Journal of Psychiatry, 161, 643-647.
https://doi.org/10.1192/bjp.161.5.643.
The measure was published formally in:
Evans, C., Searle, Y., & Dolan, B. (1998). Two new tools for the assessment of multi-impulsivity: the “MIS” and the “CAM”. European Eating Disorders Review, 6, 48–57.
Feelings and Behaviours questionnaire and to this checklist for clinicians.
Rationale and use
The drive behind the checklist was to encourage clinicians and researchers to pay more attention to the nature, phenomenology, of “impulsive” behaviours as our impression was that they were noted, and designated “impulsive” or not, very unsystematically and often in a way that opened the client up to unthoughtful and sometimes judgemental categorisation.
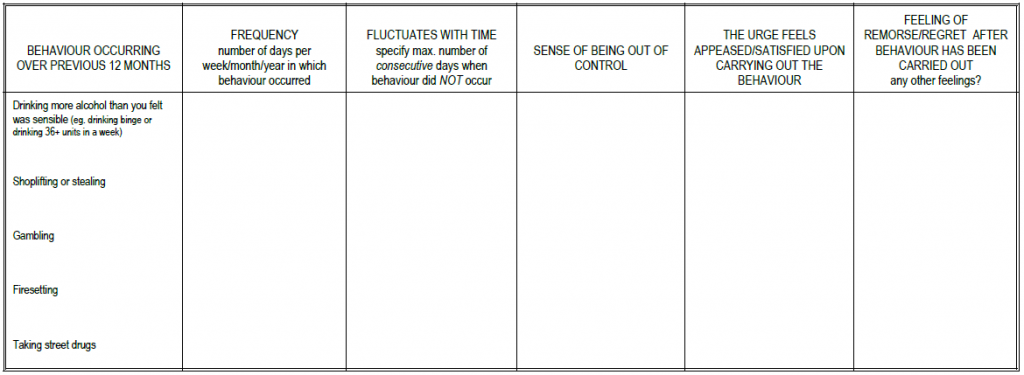
The measure fits on two sides of paper and has three blocks. This is the first block which is focused on bulimic behaviours, typically binge eating.

The aim was to create a simple and standardisable recording of the behaviour and associated feelings and experiences. The first column, a compound column, notes frequency and how much that varies, week on week. We believed, I think reasonably, that both the frequency/intensity, and the variability of that, were clinically important.
The second column notes whether there are substantial periods (rather arbitrarily, a mimimum of a month) in which it doesn’t happen. This is partly, fairly obviously, another marker of severity but not simple so as this was also to address Prof. Lacey’s idea that people with bulimia, or with binge eating problems, fell into two groups: one who only had these problems, and another group, who would probably now be put in the Borderline (DSM) or Emotionally Unstable (ICD) “personality disorder” categories who might move from one impulsive behaviour to another: Hubert’s “multi-impulsive bulimia”. (I am putting scare quotes around things here because my ambivalence about the dangers of pathologising and clinical labels, but also about the dangers of minimising the struggles many people have with these issues and the ways in which these are more trait than state phenonmena for them.)
Then there are three columns addressing what I felt to be the much neglected internal aspects that might, or might not, go with the behaviours.
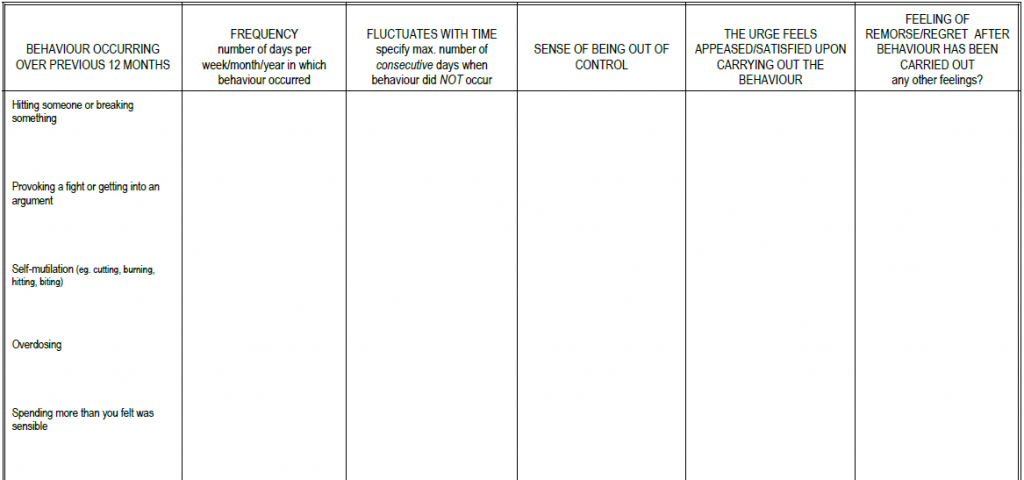
Those last three columns continue through the remaining blocks of the checklist but here headings in the first column prompt to ask about a full spread of possible problem behaviours and the frequency columns are less detailed and less specific about time course as we felt the timing that made sense for bingeing didn’t fit so well for this diversity of issues.
That continues on the second page.
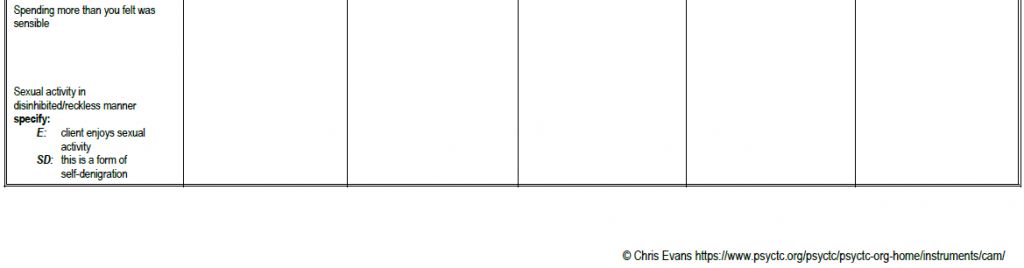
and the last category was about sexual activity where we felt the issue of predominant valency of feelings needed to be noted …
I’m not sure whether the checklist has ever been used in any systematic way. Looking back at after about twenty years, I feel a bit sad that I didn’t find time and energy to do more with it myself or to promote it a bit more as my subsequent experiences, particularly when I moved out of forensic work, were that many, probably most, mental health workers remain very casual about exploring these behaviours with clients.
That’s not to say that some mechanical working through of this checklist would necessarily be any better than largely neglecting the detail here, but I think learning from the checklist might lead to more helpful alliances with clients wanting help to change.
Copyright/licensing
The questionnaire is copyright but I am happy for anyone to use it and it is released here under a Creative Commons Atribution-NoDerivatives license . I would prefer if you didn’t make a profit out of it as my belief has always been that mental health measures should be a not for profit realm, however, in the interests of more open access the license doesn’t proscribe profiting from republishing it (but I can’t see that there’s much to be made from that as it will always be available for free!). The conditions of the licence are:
- You can change the physical nature of the questionnaire and cosmetics/aesthetics (and will probably want to do that as the versions below aren’t beautiful). I am happy for anyone to translate it and I don’t think translating a professionals’ checklist needs the rigorous work on the translation that is needed to translate a self-report questionnaire safely but please contact me if you have, or are about to, translate it.
- my copyright is clearly marked on it and this statement is made available with the original if you are giving it someone else who might use it.
I would be very grateful if you would inform me if you are using it, I’m always interested to hear if people are using it and what they’re doing with it.
Downloading
Versions mounted here:
[download id=”515″ template=”button”]
[download id=”517″ template=”button”]
[download id=”513″ template=”button”]
[download id=”506″ template=”button”]